Summertime is here and it is the time of poolside barbecues, which may consist of consuming delicious burgers and alcoholic beverages and sodas for some. In the city, I have been getting many consults for males complaining of acute joint pain, redness and swelling in the big toe as well as other joints in the fingers, elbows, and knees. Without much diagnostic evaluation, I know for many of these individuals the diagnosis is GOUT!!
WHAT IS GOUT?
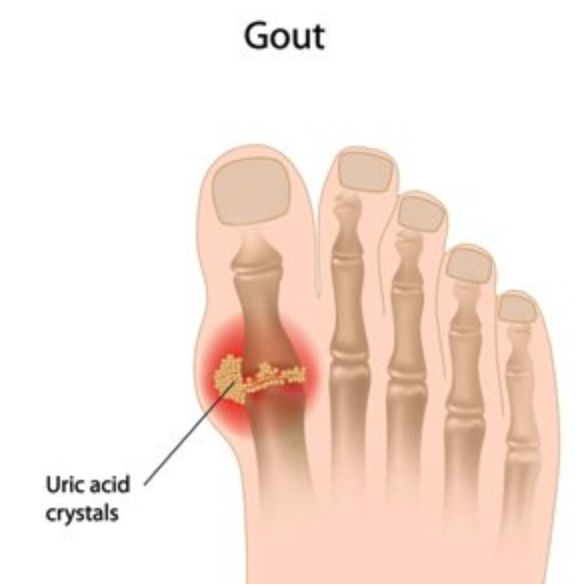
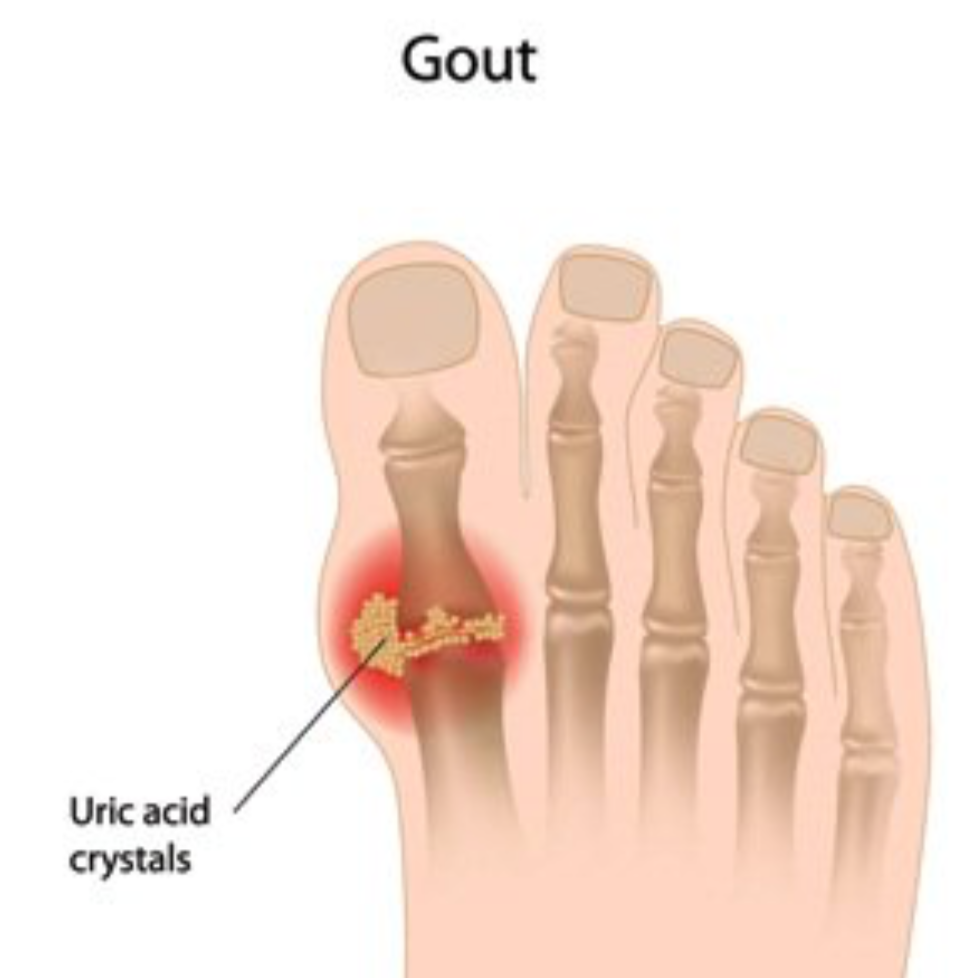
Gout is a form of inflammatory arthritis that develops in some people who have high levels of uric acid in the blood. The uric acid can crystallize and precipitate in the joint and cause sudden, severe episodes of pain, redness, warmth
I was surprised to learn that gout was actually first identified by the Egyptians and then Hippocrates in the BC era and called “The Unwalkable Disease” in the past, because of the immense joint pain and inflammation in the toes/feet. The disease was also called the “Disease of Kings” because it was associated with people living affluent lifestyles and consuming rich foods and excessive alcohol.

PERSONAL STORY
COMMON SYMPTOMS
- Acute joint pain is usually severe within the first 12-24 hours after the attack begins but pain can subside and linger for days and weeks
- Warmth
- Redness
- Swelling
- Decreased joint mobility
WHY DOES AN ATTACK HAPPEN?
Gout occurs when uric acid level accumulates in the body and then is converted to urate crystals. When the crystals deposit in the joints, inflammation occurs. We all have uric acid in our bodies that is processed and filtered by our kidneys. Uric acid can be produced when purines are broken down from foods and from natural substances in our body. Under normal circumstances, the uric acid will dissolve in
RISK FACTORS TO CONSIDER
- Diet- Certain foods have higher purine content and promote higher uric acid levels
- Red Meat/Steak
- Quail, venison
- Shellfish, sardines, herring, codfish, trout
- Scallops
- Alcoholic beverages especially beer
- High fructose drinks (soda)
- Medical Diagnosis
- Uncontrolled High Blood Pressure
- Diabetes
- Kidney Disease (especially if on dialysis)
- Metabolic Syndrome (Insulin resistance, obesity
and - Heart Disease
- Family History of gout, Kidney Stone
- Recent Surgery hospitalization or trauma
- Dehydration
- Male Sex
- Age- Males most likely develop gout in
mid 30s-age - Postmenopausal women are at risk.
- Medication
- Thiazide diuretics (Hydrochlorothiazide) used to treat hypertension
- Cyclosporine used for psoriasis and other conditions
- Immunosuppressant drugs used for organ transplant patients
- Low dose aspirin
- Nicotinic acid
- Drugs used to treat tuberculosis (Pyrazinamide and
Etambutol ) - Obesity- Your body produces more uric acid
WHY DO WE CARE IF OUR URIC ACID LEVELS REMAIN ELEVATED?
1) Development of chronic inflammatory gouty arthritis. Chronic gout can lead to bone damage and joint destruction.
2) Kidney stones – Uric acid can deposit in the urinary tract
3) Tophi- Deposits of urate crystals under the skin forming nodules in the feet, elbows, ankles, hands, Achilles tendon.
4) Possible link with cardiovascular disease and mortality
5) Association with Metabolic syndrome
WHAT WILL YOUR RHEUMATOLOGIST DO?
- Take
a clinical - Get blood tests looking for uric acid level, white blood cell count, kidney function, and inflammation markers
- Sometimes if a joint is markedly swollen, an arthrocentesis or joint fluid aspiration procedure may be performed. The joint fluid will then be sent to a lab to be analyzed for crystals and to rule out infection.
- Xrays
- In recent years, musculoskeletal ultrasound and
Dual energy CT scan are being more often used to detect uratectystals in the joint even if there is no acute inflammation.
WHEN SHOULD TREATMENT BE INITIATED?
Your physician may place you on medication if you are experiencing several attacks a year, attacks are becoming more frequent, there are complications from high uric acid levels or if there is bone damage on musculoskeletal tests.
MEDICATION TREATMENT OPTIONS INCLUDE:
- Colchicine- helps with acute attack and prevention
Non steroidal Anti inflammatory acute attack.- Oral Steroids and/or local steroid injections can help with an acute attack.
- Uric
acid lowering agents- Xanthine oxidase inhibitors which reduce the level of uric acid the body makes - Allopurinol
- Febuxostat (Uloric)
- Uricosurics (Probenecid, Lesinurd) help the kidneys remove the uric acid from the body more efficiently. Urine acid level is increased.
- Pegloticase ( Krystexxa)- IV infusion to treat refractory severe chronic gout by reducing uric acid levels and dissolving uric acid crystals.
Important note:
With all of the above medications, please discuss with your physician whether the medication is the right choice for you. Patients with heart failure, Diabetes, Kidney disease and Ulcer disease need to be cautious with treatment choices. All of these medications have side effects and your liver, kidney, and cell counts have to be regularly monitored by a physician.
PREVENTION TIPS
- Limit alcoholic consumption- Try an unsweetened mocktail this summer!
- Stay hydrated!! Carry your water bottle with you all the time!
- Limit high fructose-sweetened beverages- Stick to plain water or water infused with cucumber or lemon!
- Avoid red meat, shellfish. I know this is difficult especially during summertime but maybe stick to a small portion of chicken (white meat) and veggies. Try that avocado roll at dinner!
- Try increasing low-fat dairy products in your regimen.
- Maintain good blood pressure and ideal body weight. Speak to your physician about what your ideal numbers are for you!
- Exercise and keep moving!!
- Try and keep
uric . Some reports have suggested that cherries/cherry extract and Vitamin C may help lower uric acid levels however more research has to be done! Other home remedies that have been reported to help are warm water with apple cider vinegar, lemon juice, turmeric, ginger, milk thistle. Again, more studies need to be conducted to evaluate efficacy in treatment.
Gout was once considered a “rich man’s disease” but we all know that this inflammatory condition can occur in any socio-economic class and in both sexes! Enjoy the summer but also keep some of the prevention tips in mind!
References:
Current Rheumatology
Arthritis Research and Therapy 2006 8 (Supp 1)
American College of Rheumatology, Mayo Clinic
Disclaimer: This blog contains my personal opinion based on personal and clinical experience, tips from trainers, health coaches and lastly research. This blog does not endorse specific treatments, procedures, products. You should always consult with a doctor, nutritionist, or other healthcare professional to discuss your own health and lifestyle goals and regimen based on your medical history. Thank you for reading!